

Where Would The Money Come From For Single Payer Healthcare
"How are you going to pay for information technology?" Unmarried-payer skeptics ofttimes ask this question in a bad-faith attempt to discredit Medicare for All. Only the answer is uncomplicated: We're already spending plenty on health care. We're only non getting our coin'due south worth.
PNHP-MN interns and medical students Conor Nath and Preethiya Sekar reviewed the evidence by analyzing a decade'south worth of post-ACA unmarried-payer financing studies during the summer of 2020 (John A. Nyman, Ph.D.; Gordon Mosser, M.D.; and Kenneth Englehart, M.D. served equally advisors). The team developed detailed infographics for each study (see beneath) besides as a primer and a PowerPoint presentation that offer an overview of their project.
PNHP will add together new financing studies to this page as they are published (well-nigh recent study appearing first). For archival links to pre-ACA analyses, land-based studies, and a succinct statement from one-time American Public Wellness Clan president Dr. Linda Rae Murray, click here.
It is too worth noting several high-contour Medicare-for-All financing plans that were released during the 2020 Democratic Principal, 1 from Sen. Elizabeth Warren and ane from Sen. Bernie Sanders (with other plans included; Medicare for All is the final item on the folio). PNHP offered comment on these proposals, hither.
Of course, the status quo is unsustainable. National health spending continues to grow at a rapid clip, year after twelvemonth after year, with the latest figures from 2019 showing a four.7% increase from 2018, to $three.8 trillion. That'due south more than than enough to finance all medically necessary intendance for every U.S. resident while totally eliminating out-of-pocket spending.
Lesser line: a single-payer national health program is non only affordable, it'due south the only affordable pick.
"Economic Effects of 5 Illustrative Single-Payer Wellness Intendance Systems"
Congressional Budget Office 2022
Title: Economical Effects of Five Illustrative Unmarried-Payer Health Care Systems
Year: 2022
Authors: Jaeger Nelson
Institution: Congressional Budget Office
Plan Analyzed: "Five illustrative options" for a single-payer national wellness program, not strictly based on existing legislation
Percent Change in National Wellness Expenditure under M4A: Ranging from a decrease of $743 billion to an increase of $290 billion in 2030
Read Report:
Economic Furnishings of V Illustrative Single-Payer Health Care Systems, Working Paper
Abstruse:
Further Reading:
- Health Justice Monitor entry by Drs. Don McCanne and Jim Kahn
- "The Authorities'due south Ain Number Crunchers Agree: We Need Medicare for All" past David Sirota and Aditi Ramaswami, Jacobin, February. 25, 2022
"How CBO Analyzes the Costs of Proposals for Unmarried-Payer Wellness Care Systems That Are Based on Medicare'due south Fee-for-Service Programme"
Congressional Upkeep Office 2020
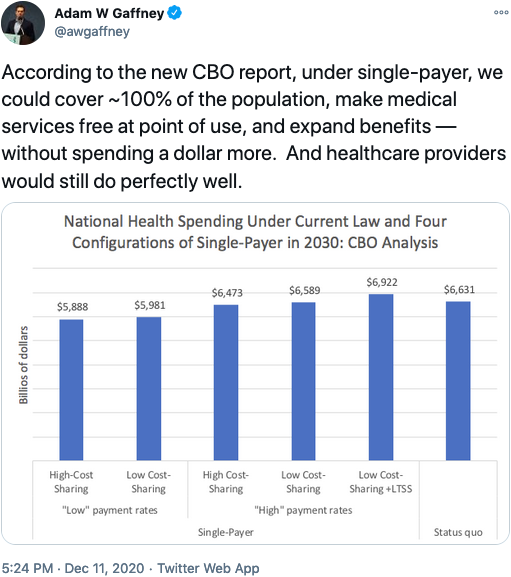
Title: How CBO Analyzes the Costs of Proposals for Single-Payer Health Intendance Systems That Are Based on Medicare'southward Fee-for-Service Program
Year: 2020
Authors: CBO's Single-Payer Health Care Systems Team
Institution: Congressional Upkeep Office
Plan Analyzed: "V illustrative options" for a single-payer national health programme, not based on H.R. 1384 or S.1129
Percent Alter in National Health Expenditure nether M4A (10-year): Ranging from a decrease of $0.vii trillion to an increase of $0.3 trillion in 2030
Read Written report:
How CBO Analyzes the Costs of Proposals for Unmarried-Payer Health Care Systems That Are Based on Medicare'southward Fee-for-Service Plan: Working Newspaper 2020-08
Summary:
Farther Reading:
- Web log by CBO Managing director Phillip Swagel
- Quote of the Day by Dr. Don McCanne
- "CBO: Medicare for All Reduces Health Spending" by Matt Bruenig, People's Policy Project
- "Utilization of health care services after large coverage expansions" series of studies debunking the merits the health care utilization would fasten under unmarried payer
- "Key Design Components and Considerations for Establishing a Single-Payer Health Intendance Arrangement" published by the Congressional Budget Function, May 2019
Congressional Hearings on 2019 Written report:
back to top
"Improving the Prognosis of Health Care in the U.s."
Yale School of Public Health 2020
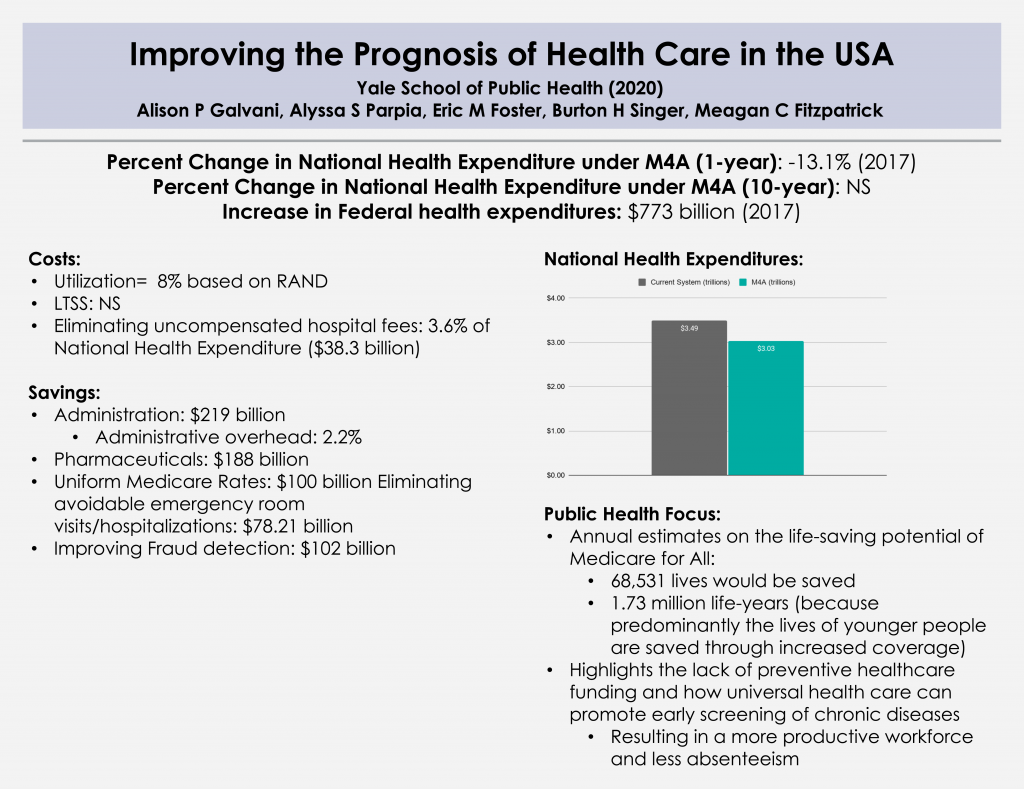
Title: Improving the prognosis of health intendance in the The states
Year: 2020
Authors: Alison P. Galvani, Alyssa Due south. Parpia, Eric One thousand. Foster, Burton H. Singer, Meagan C. Fitzpatrick
Institution: Yale School of Public Wellness
Funding Source: N/A
Programme Analyzed: S. 1804 Medicare for All Human activity of 2017
Percent Alter in National Wellness Expenditure under M4A (1-year): -13.ane% (2017)
Percent Modify in National Health Expenditure nether M4A (10-twelvemonth): NS
Increase in Federal health expenditures: $773 billion (2017)
Read Study:
Improving the prognosis of wellness care in the The states
Written report Abstract:
Although health intendance expenditure per capita is higher in the Us than in any other country, more than 37 million Americans practice non have health insurance, and 41 million more have inadequate access to care. Efforts are ongoing to repeal the Affordable Care Deed which would exacerbate health care inequities. Past contrast, a universal system, such as that proposed in the Medicare for All Deed, has the potential to transform the availability and efficiency of American wellness intendance services. Taking into account both the costs of coverage expansion, and the savings that would be achieved through the Medicare for All Act, nosotros calculate that a unmarried-payer, universal health intendance organisation is likely to lead to a 13% savings in national health-care expenditure, equivalent to more than than US$450 billion annually (based on the value of the U.s.a.$ in 2017). The entire organization could be funded with less financial outlay than is incurred by employers and households paying for health care premiums combined with existing authorities allocations. This shift to single-payer health care would provide the greatest relief to lower-income households. Furthermore, we estimate that ensuring health care access for all Americans would salvage more than 68,000 lives and 1.73 million life-years every year compared with the condition quo.
Overview:
- In early 2020, Alison Galvani published a price-analysis of the Senate Medicare for All beak, S. 1804. Of note, Galvani served as an "informal unpaid adviser" to the writers of this detail bill.
- The Yale study focuses on:
- Savings from reduced fees for hospital and clinical services, unified system for billing and administration, pharmaceutical price negotiation
- The cost of expansion of coverage and services
- Financing programme furnishings on employers and households
- Public health approach to guess "life-years" saved by Medicare for All
- Positive spillovers from emphasizing preventive services
- Creation of a Tool that can model costs/savings also as revenue generation
Farther Reading:
SHIFT Tool allowing users to modify inputs and assumptions
back to acme"Projected costs of unmarried-payer healthcare financing in the U.s.: A systematic review of economic analyses"
PLOS Medicine 2020
Championship: Projected costs of unmarried-payer healthcare financing in the Us: A systematic review of economic analyses
Year: 2020
Author: Christopher Cai, Jackson Runte, Isabel Ostrer, Kacey Drupe, Ninez Ponce, Michael Rodriguez, Stefano Bertozzi, Justin Southward. White, James Grand. Kahn
Institution: Academy of California, San Francisco
Plan Analyzed: Economic analyses of 22 unmarried-payer plans published over the past 30 years
Percentage Change in National Health Expenditure nether M4A: -3.46% (median savings for the 19 of 22 analyses that predicted net savings)
Read Study:
Projected costs of single-payer healthcare financing in the United States: A systematic review of economical analyses
Report Abstruse:
Groundwork: The United states of america is the only loftier-income nation without universal, government-funded or -mandated health insurance employing a unified payment system. The US multi-payer system leaves residents uninsured or underinsured, despite overall healthcare costs far above other nations. Single-payer (often referred to as Medicare for All), a proposed policy solution since 1990, is receiving renewed press attention and popular back up. Our review seeks to assess the projected cost impact of a unmarried-payer approach.
Methods and findings: We conducted our literature search between June i and December 31, 2018, without first date restriction for included studies. We surveyed an expert panel and searched PubMed, Google, Google Scholar, and preexisting lists for formal economic studies of the projected costs of single-payer plans for the U.s.a. or for individual states. Reviewer pairs extracted data on methods and findings using a template. We quantified changes in full costs standardized to percentage of contemporaneous healthcare spending. Additionally, we quantified toll changes by subtype, such as costs due to increased healthcare utilization and savings due to simplified payment administration, lower drug costs, and other factors. We farther examined how modeling assumptions afflicted results. Our search yielded economical analyses of the cost of 22 single-payer plans over the past xxx years. Exclusions were due to inadequate technical data or bold a substantial ongoing office for private insurers. Nosotros found that 19 (86%) of the analyses predicted cyberspace savings (median net result was a savings of 3.46% of full costs) in the kickoff twelvemonth of program performance and 20 (91%) predicted savings over several years; anticipated growth rates would event in long-term cyberspace savings for all plans. The largest source of savings was simplified payment administration (median 8.eight%), and the best predictors of net savings were the magnitude of utilization increase, and savings on administration and drug costs (R2 of 0.035, 0.43, and 0.62, respectively). Only drug cost savings remained significant in multivariate assay. Included studies were heterogeneous in methods, which precluded us from conducting a formal meta-analysis.
Conclusions: In this systematic review, we establish a high degree of analytic consensus for the fiscal feasibility of a single-payer approach in the US. Bodily costs will depend on programme features and implementation. Future research should refine estimates of the effects of coverage expansion on utilization, evaluate provider authoritative costs in varied existing single-payer systems, analyze implementation options, and evaluate US-based single-payer programs, as available.
Further reading:
- UCSF press release
- Quote of the Day by Dr. Don McCanne
"From Incremental to Comprehensive Wellness Insurance Reform: How Various Reform Options Compare on Coverage and Costs"
The Urban Establish 2019
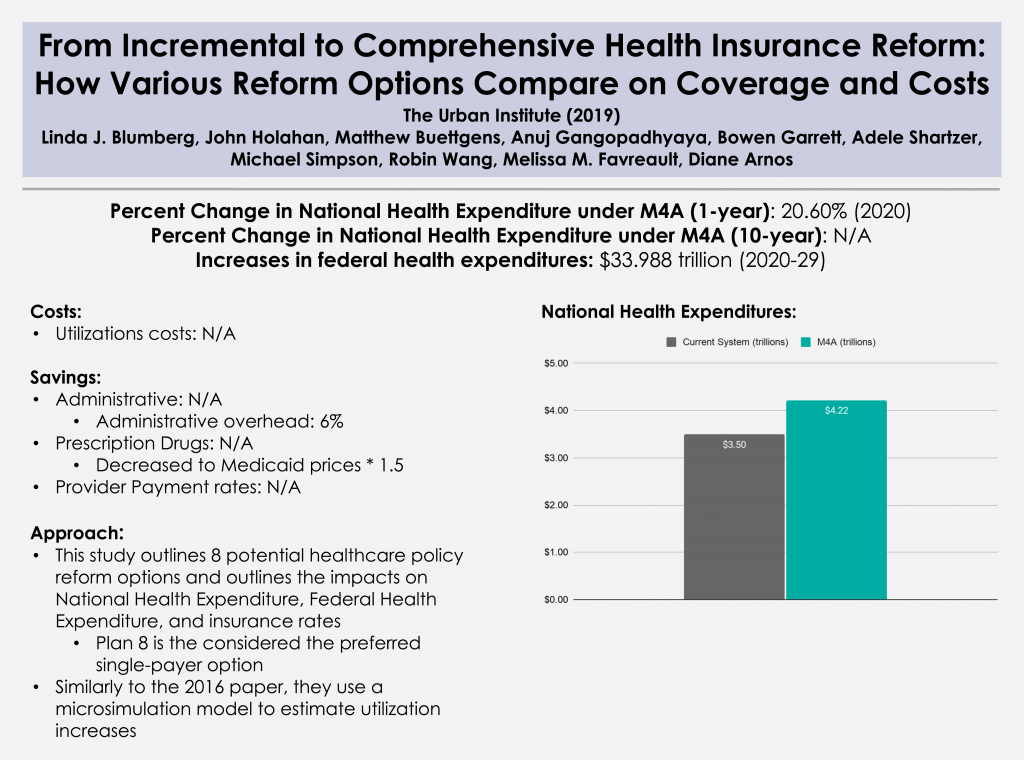
Title: From Incremental to Comprehensive Health Insurance Reform: How Various Reform Options Compare on Coverage and Costs
Year: 2019
Author: Linda J. Blumberg, John Holahan, Matthew Buettgens, Anuj Gangopadhyaya, Bowen Garrett, Adele Shartzer, Michael Simpson, Robin Wang, Melissa M. Favreault, and Diane Arnos
Institution: Urban Institute
Funding Source: The Democracy Fund
Program Analyzed: "Reform 8"
Percent Alter in National Wellness Expenditure under M4A (1-year): twenty.6% (2020)
Percent Alter in National Health Expenditure under M4A (10-year): NS
Increases in federal health expenditures: $33.988 trillion (2020-29)
Read Study:
From Incremental to Comprehensive Health Insurance Reform: How Diverse Reform Options Compare on Coverage and Costs
Abstract:
Policymakers, including candidates in the 2020 presidential campaign and members of Congress, have proposed a variety of options to address the shortcomings of the current wellness care system. These range from improvements to the Affordable Care Act to robust single-payer reform.
There are numerous challenging trade-offs when choosing an approach to health care reform, including covering the uninsured, improving the affordability of health care, and raising the government funding required to implement them. The public and policymakers akin need more information most the potential furnishings of various health reform proposals.
This study, funded by the Commonwealth Fund, analyzes eight wellness intendance reforms and their potential furnishings on health insurance coverage and spending. Each of the analyzed reform proposals makes health insurance considerably more affordable by reducing people's premiums and cost sharing. Some reforms besides reduce U.s. health care costs, and all require boosted federal dollars.
Overview:
- This report is unique in that it outlines 8 potential health care policy reform options, and and so outlines impacts on national wellness expenditures, federal health expenditure, and insurance rates. Information technology utilizes the aforementioned microsimulation arroyo that the Urban constitute utilized in its 2016 paper.
- Reforms considered by this paper include those that:
- Build on the ACA
- Reform i: Enhanced financial assist
- Reform 2: Federal individual mandate and STLD prohibitions
- Reform iii: Filling the Medicaid eligibility gap
- Reform 4: Public option and/or capped provider payment rates
- Reform 5: CARE, no ESI firewall
- Reform half dozen: Further enhanced financial help
- Replace the ACA
- Reform 7: Unmarried-payer lite
- Reform 8: Single-payer enhanced
- Build on the ACA
PNHP Response:
PNHP co-founders Drs. David Himmelstein and Steffie Woolhandler institute that "the Urban Institute analysis grossly underestimates the authoritative savings nether unmarried payer, and projects increases in the number of dr. visits and hospitalizations that far exceed the capacity of doctors and hospitals to provide this added care." Their full critique hither, and a QOTD response from Dr. Don McCanne, including comments from PNHP president Dr. Adam Gaffney, here.
Farther Reading:
Comparing Health Insurance Reform Options: From "Building on the ACA" to Unmarried Payer
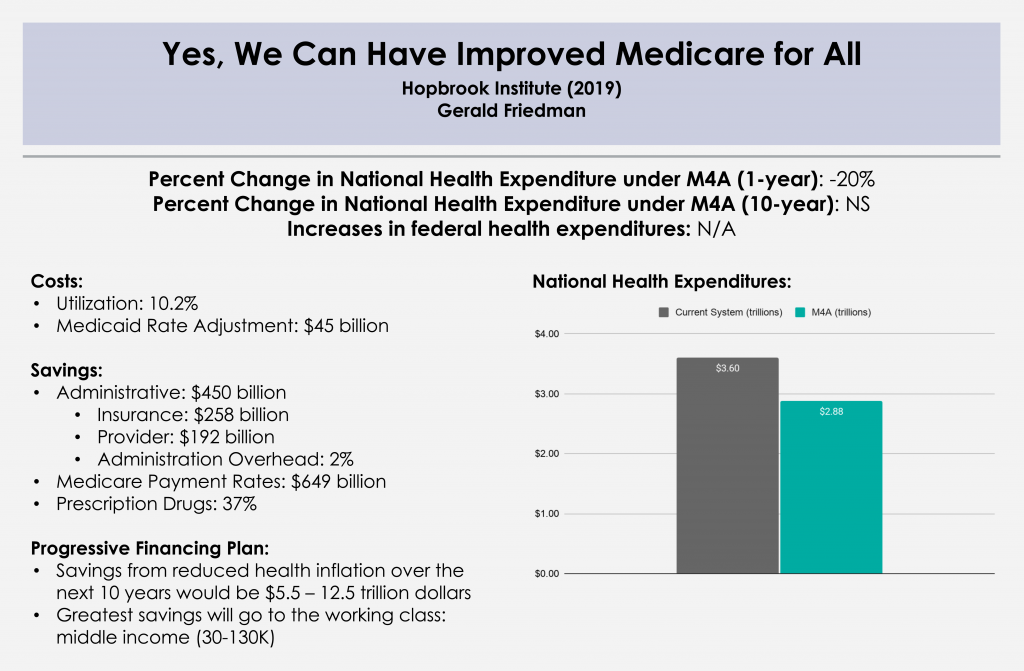
dorsum to top"Yes, We Tin can Take Improved Medicare for All"
Hopbrook Found 2019
Championship: Yeah, We Tin can Have Improved Medicare for All
Year: 2019
Writer: Gerald Friedman
Establishment: Academy of Massachusetts at Amherst
Funding Source: Hopbrook Establish
Plan Analyzed: H.R. 676
Percent Change in National Health Expenditure under M4A (i-year): -20.0% (2019)
Per centum Change in National Health Expenditure under M4A (10-year): -20.vi% (2019-28)
Read Report:
Yes, We Tin Have Improved Medicare for All
Abstract:
Growing public back up for universal health coverage through a public programme has provoked increasing attention to the question of how to finance such a program. In that location should not be any controversy about our ability to pay for universal health care. Given the nearly universal agreement that the current health-care organisation involves administrative waste material and monopoly pricing, a system that would be more efficient and would reduce both should certainly be affordable. Studies finding higher costs for universal coverage programs have reached their conclusions by acknowledging efficiency savings but dismissing them past emphasizing, even exaggerating, the higher costs of providing better admission to health care. Such studies provide a poor guide to the possibilities for an overhaul of our health-intendance finance system. In this newspaper, I discuss the financing of a universal wellness-intendance program, beginning with a word of current projected spending and the savings to be achieved through authoritative efficiency and reducing monopoly pricing. Next, I outline increased spending associated with universal coverage through covering the uninsured and reducing barriers to admission. I consider the net cost of universal coverage, afterward taking account of savings and the cost of extending and improving coverage, under various scenarios with culling immediate savings and savings over time. Finally, I discuss sources of funding for such a program, beginning with public funds already committed and including possible boosted sources of revenue. I develop funding plans under a variety of assumptions regarding the course of the single-payer organisation, and under alternative assumptions regarding acquirement sources. This work shows that compared with the current organization of health-intendance finance, a program of Improved Medicare for All could save Americans over $1 trillion in the first year, and savings could increase over time. Because some of the savings would be returned to health care through programs of universal coverage and improved access, net savings could exist over $700 billion in the first year, rise over the next decade. Depending on the assumptions made and the program details, full fiscal savings, subsequently taking business relationship of program improvements, would come to $10 trillion or more than over the next decade, on top of gains in quality of life and reduced mortality through universal admission. A diversity of models are compared, with varying assumptions of the magnitude of administrative savings and savings through reduced monopoly rents, as well equally savings from bending the toll bend and maintaining some price-sharing. Overall, the 10-year national savings on health-care expenditures range from a low of over $half-dozen trillion to a high of over $thirteen trillion. In every model tested, Improved Medicare for All is cheaper than the current system even while providing improved health care.
Overview:
Comprehensive price analysis conducted past Gerald Friedman updating his previous work on the subject with similar considerations for financing options.
- Section 1: Current spending and waste
- Administrative savings in provider offices
- Savings from pricing at Medicare negotiated rates
- Drugs and medical devices
- Hospital and physician practices
- Section 2: Additional spending with universal coverage
- Medicare premiums
- Cost of universal coverage
- Cost of eliminating barriers to access
- Section 3: Total Spending with Medicare for All
- Section four: Paying for Medicare for All
- Available revenues
- New revenues
- Conclusion: We tin beget Improved Medicare for All
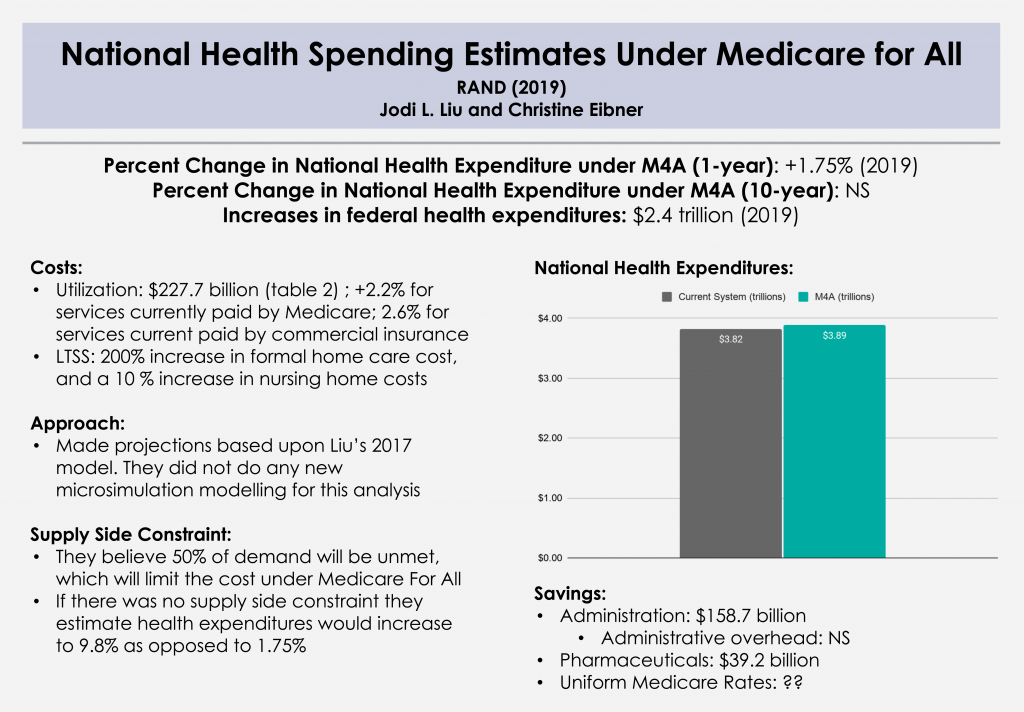
"National Health Spending Estimates Nether Medicare for All"
RAND 2019
Championship: National Health Spending Estimates Under Medicare for All
Twelvemonth: 2019
Authors: Jodi L. Liu and Christine Eibner
Institution: RAND
Funding Source: Modeled after H.R. 1384
Plan Analyzed: S. 1782 / H.R. 1200
Percent Change in National Wellness Expenditure nether M4A (1-year): +1.75% (2019)
Percentage Change in National Wellness Expenditure under M4A (10-twelvemonth): NS
Increases in federal health expenditures: $ii.4 trillion (2019)
Read Study:
National Wellness Spending Estimates Under Medicare for All
Study Abstruse:
We estimate that total health expenditures under a Medicare-for-All plan that provides comprehensive coverage and long-term care benefits would be $3.89 trillion in 2019 (assuming such a plan was in identify for all of the year), or a 1.eight per centum increase relative to expenditures under current law. This estimate accounts for a variety of factors including increased need for wellness services, changes in payment and prices, and lower authoritative costs. We as well include a supply constraint that results in unmet demand equal to 50 percent of the new demand. If in that location were no supply constraint, we estimate that total health expenditures would increase by 9.8 percent to $4.twenty trillion.
While the ane.8 percent increase is a relatively small change in national spending, the federal government's health care spending would increase essentially, rising from $1.09 trillion to $3.50 trillion, an increase of 221 per centum.
Overview:
- An update washed past extrapolating projections from the microsimulation modelling in the 2016 RAND study. No new modelling was undertaken for this analysis.
- This study considers:
- Increased need for medical services and long-term care services and supports (LTSS)
- Savings from all-payer rates for services, prices for drugs and devices, administrative costs
- Supply-side constraints for services
- Level of financing needed for Medicare For All
PNHP Response:
Regarding increased utilization, we would highlight three studies from 2019 that found large-scale coverage expansions in the U.s. (Medicare/Medicaid in the belatedly 1960s and the ACA in the early on 2010s) did not lead to a society-wide increase in hospitalizations or doctor visits, and that large-scale expansions in other nations also did non crusade a fasten in utilization. (See "Utilization of health care services after large coverage expansions.")
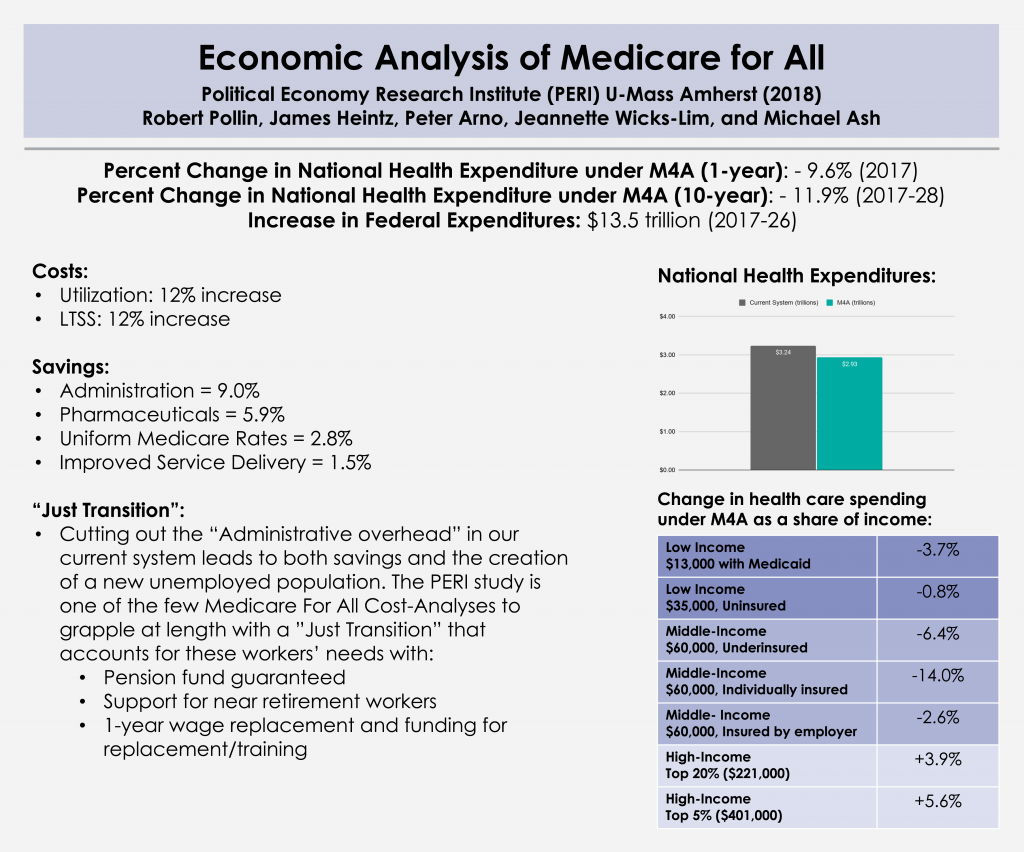
back to pinnacle"Economic Assay of Medicare for All"
Political Economic system Research Constitute (PERI) 2018
Championship: Economic Assay of Medicare for All
Year: 2018
Author: Robert Pollin, James Heintz, Peter Arno, Jeannette Wicks-Lim, and Michael Ash
Establishment: Political Economy Research Institute (PERI) U-Mass Amherst
Funding Source: California Nurses Association/National Nurses United
Plan Analyzed: S. 1804 Medicare for All Act of 2017
Percent Change in National Health Expenditure under M4A (one-yr): -9.6% (2017)
Percent Change in National Health Expenditure under M4A (x-year): -11.9% (2017-26)
Increase in Federal health expenditures: $i.35 trillion (2017-26)
Read Study:
PERI – Economic Assay of Medicare for All
Study Abstract:
This study by PERI researchers Robert Pollin, James Heintz, Peter Arno, Jeannette Wicks-Lim and Michael Ash presents a comprehensive analysis of the prospects for a Medicare-for-All health care arrangement in the United States. The almost primal goals of Medicare for All are to significantly meliorate wellness intendance outcomes for anybody living in the United states while also establishing effective cost controls throughout the health care system. These 2 purposes are both doable. As of 2017, the U.S. was spending most $3.24 trillion on personal wellness care—nearly 17 percent of total U.S. Gdp. Meanwhile, ix per centum of U.S. residents had no insurance and 26 pct were underinsured—they were unable to admission needed care because of prohibitively high costs. Other loftier-income countries spend an average of about twoscore percent less per person and produce better health outcomes. Medicare for All could reduce total health intendance spending in the U.Due south. by nearly ten pct, to $ii.93 trillion, while creating stable admission to good intendance for all U.S. residents.
Overview:
- The PERI study is a lengthy and comprehensive cost-analysis study. The authors explicate their assumptions and counterfactuals at length and bear witness their calculations in a very piece of cake-to-follow format.
- The Report contains vii sections:
- Chapter ane: Underscores why affordable health care tin can amend health outcomes
- Chapters 2-3: Identifies sources of costs and savings
- Chapter four: Financing Plans for Medicare For All
- Chapter v: Furnishings of financing plans on families (based on income) and businesses (small-scale, medium, and big)
- Affiliate vi: Considers the logistics and the costs of transitioning from our current system to a single-payer system ("Merely Transition")
- Chapter 7: Estimates the furnishings of Medicare for All on health care spending as a share of US GDP, and other macroeconomic impacts
PNHP Response:
PNHP co-founders Drs. Steffie Woolhandler and David Himmelstein, and PNHP president Dr. Adam Gaffney, submitted a reviewer cess of the PERI study. They notation that the PERI analysis may understate administrative savings, but overall find it to exist a "highly credible economic analysis."
Further Reading:
Facing job loss with But Transition (KHN)
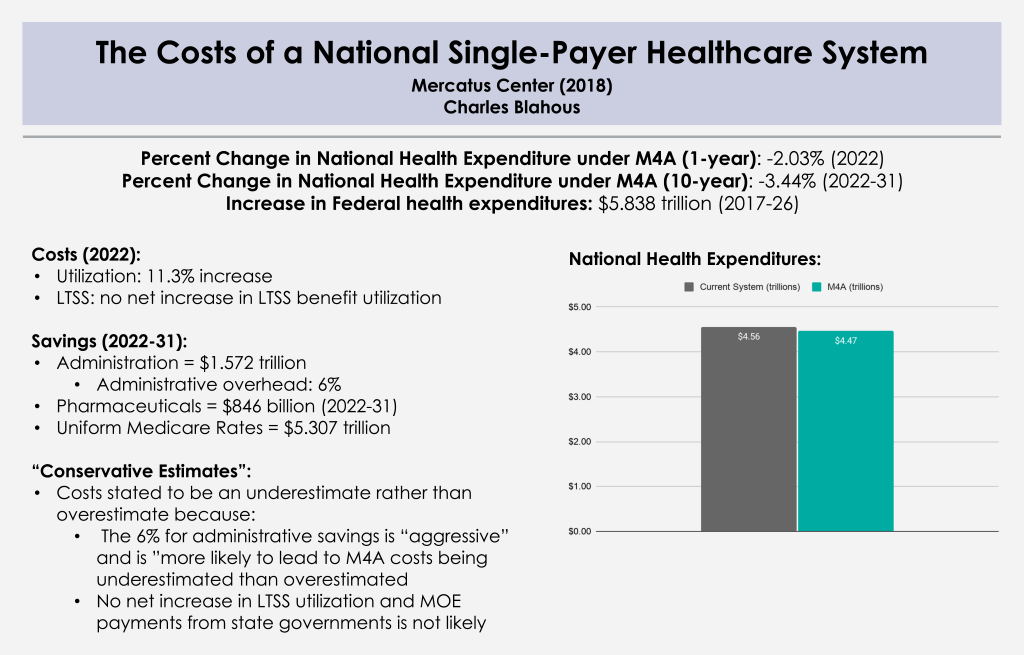
dorsum to top"The Costs of a National Single-Payer Healthcare System"
Mercatus Middle 2018
Title: The Costs of a National Single-Payer Healthcare System
Yr: 2018
Authors: Charles Blahaus
Establishment: Mercatus Center
Funding Source: Koch
Plan Analyzed: S. 1804 Medicare for All Act of 2017
Percent Change in National Health Expenditure nether M4A (1-year): -2.03% (2022)
Per centum Change in National Health Expenditure under M4A (x-year): -three.44% (2022-31)
Increase in Federal health expenditures: $five.838 trillion (2017-26)
Read Written report:
The Costs of a National Single-Payer Healthcare Organisation
Study Abstract:
The leading electric current nib to establish unmarried-payer wellness insurance, the Medicare for All Act (M4A), would, nether conservative estimates, increase federal budget commitments past approximately $32.half-dozen trillion during its showtime 10 years of full implementation (2022–2031), assuming enactment in 2018. This projected increase in federal health care commitments would equal approximately 10.7 percent of Gdp in 2022, rising to near 12.7 percentage of Gdp in 2031 and farther thereafter. Doubling all currently projected federal individual and corporate income tax collections would exist insufficient to finance the added federal costs of the plan. It is probable that the actual price of M4A would be substantially greater than these estimates, which assume significant authoritative and drug price savings under the plan, and also assume that health care providers operating under M4A will be reimbursed at rates more than than 40 percent lower than those currently paid past private health insurance.
Overview:
- The Mercatus Report focuses on national health expenditures (NHE), but places particular emphasis on federal health expenditures.
- The Written report focuses on:
- An overview of the findings and rationale for why Blahaus believes his guess is an "underestimate"
- Particular Increased Need and Utilization assumptions and Long Term Services and Supports (LTSS)
- Savings from Provider Payment Reductions, Drug Costs, Administrative Savings. Blahaus underscores that all of these savings volition likely not be accomplished considering his estimates crave a perfect transition from policy to practice. (Authoritative Tasks, Prescription Drug Negotiation, etc) operate their optimal capacity/efficiency
- Furnishings on NHE and the Federal Budget, expressing skepticism virtually financing plans despite not laying out any particular financing plans
- Appendix with Fiscal Furnishings of unlike scenarios under Medicare for All
PNHP Response:
PNHP co-founders Drs. David Himmelstein and Steffie Woolhandler critique the Mercatus reports as "ideology masquerading every bit wellness economics."
Further Reading:
- "SinglePayerGate" misses the indicate: (Voice)
- Blahous Rebuttal: (e21)
"The Sanders Unmarried-Payer Health Intendance Plan: The Effect on National Wellness Expenditures and Federal and Private Spending"
The Urban Constitute 2016
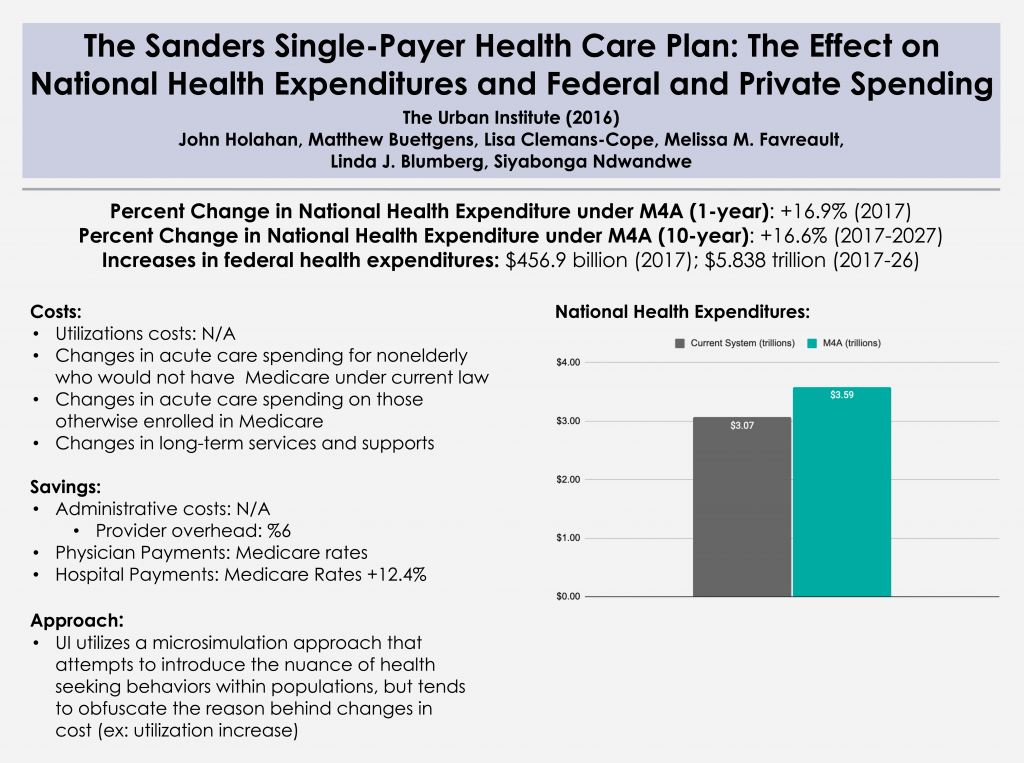
Championship: The Sanders Single-Payer Health Care Plan: The Event on National Health Expenditures and Federal and Private Spending
Yr: 2016
Author: John Holahan, Lisa Clemans-Cope, Matthew Buettgens, Melissa Favreault, Linda J. Blumberg, and Siyabonga Ndwandwe
Institution: Urban Institute
Funding Source: Due north/A
Plan Analyzed: Bernie Sanders' 2016 campaign proposal (eventually became Due south. 1804 Medicare for All Act of 2017)
Percent Change in National Health Expenditure nether M4A (1-year): 16.9% (2017)
Percentage Modify in National Wellness Expenditure under M4A (10-yr): 16.six% (2017-26)
Increases in federal health expenditures: $456.9 billion (2017)
Read Study:
The Sanders Unmarried-Payer Health Care Program
Abstract:
Presidential candidate Bernie Sanders proposed a single-payer system to replace all current health coverage. His system would embrace all medically necessary intendance, including long-term intendance, without cost-sharing. We judge that the arroyo would decrease the uninsured by 28.3 million people in 2017. National health expenditures would increase past $6.6 trillion between 2017 and 2026, while federal expenditures would increase past $32.0 trillion over that period. Sanders's acquirement proposals, intended to finance all health and nonhealth spending he proposed, would raise $15.3 trillion from 2017 to 2026—thus, the proposed taxes are much as well low to fully finance his wellness plan.
Overview:
- 2016 study washed by the Urban Constitute utilizing a microsimulation approach to deport a cost analysis of the Sanders Medicare for All proposal from the 2016 presidential primary in dissimilarity to projection studies that had been done up to that point.
- This study considers how cost would be affected by:
- Acute healthcare spending increases by not-elderly individuals who would non otherwise be enrolled in Medicare
- Acute healthcare spending increases past those who would otherwise be enrolled in medicare under currently law
- Increase in utilization costs for long term services and supports
- This study discusses
- Assumptions that tend to over/underestimate costs when because M4A.
Farther Reading:
- PNHP Response
- Urban Institute Response to PNHP
- PNHP Counter-Response
- Gordon Mosser Critical Review and annotate by Dr. Don McCanne
"An Analysis of Senator Sanders' Single-Payer Plan"
Emory University 2016

Championship: An Analysis of Senator Sanders Unmarried Payer Plan
Yr: 2019
Author: Kenneth Thorpe
Institution: Emory University
Programme Analyzed: S. 1129
Increases in federal health expenditures: $1.9 trillion (2017) and $24.6 trillion (2017-26)
Read Report:
An Analysis of Senator Sanders'due south Single Payer Plan
Abstract:
Senator Sanders has proposed eliminating private health insurance and the exchanges created through the Affordable Care Act and replacing it with a universal Medicare program with no toll sharing. The programme would shift virtually all health care spending from private and public sources today onto the federal budget. The entrada estimates his plan would cost an average of $one.38 trillion per year over the side by side decade. They outline a variety of payroll and income tax increases, college taxes for capital letter gains and dividends, taxes on estates of high income households and eliminate revenue enhancement breaks that subsidize health insurance. Collectively he claims these taxes fully pay for the costs of the unmarried payer program. The analysis presented below still estimates that the average annual cost of the plan would be approximately $2.five trillion per year creating an average of over a $1 trillion per twelvemonth financing shortfall. To fund the plan, payroll and income taxes would have to increment from a combined 8.four pct in the Sanders plan to 20 percent while also retaining all remaining tax increases on capital gains, increased marginal tax rates, the estate tax and eliminating tax expenditures. The plan would create enormous winners and losers even with the more generous benefits with respect to what households and businesses pay today compared to what they would pay under a unmarried payer plan. Overall, over lxx percent of working privately insured households would pay more under a fully funded single payer program than they do for health insurance today.
Overview:
This study is unique considering information technology primarily focuses on the increase in federal health care spending and how this increment might be financed.
This study considers:
- The bear on of increased payment rates for current Medicare/Medicaid beneficiaries.
- Financing mechanisms for increased federal spending.
- Populations that would be "at-chance" based on proposed financing mechanisms.
Farther Reading:
Gordon Mosser Critical Review and comment by Dr. Don McCanne
dorsum to elevation"Exploring Single-Payer Alternatives for Health Care Reform"
RAND 2016
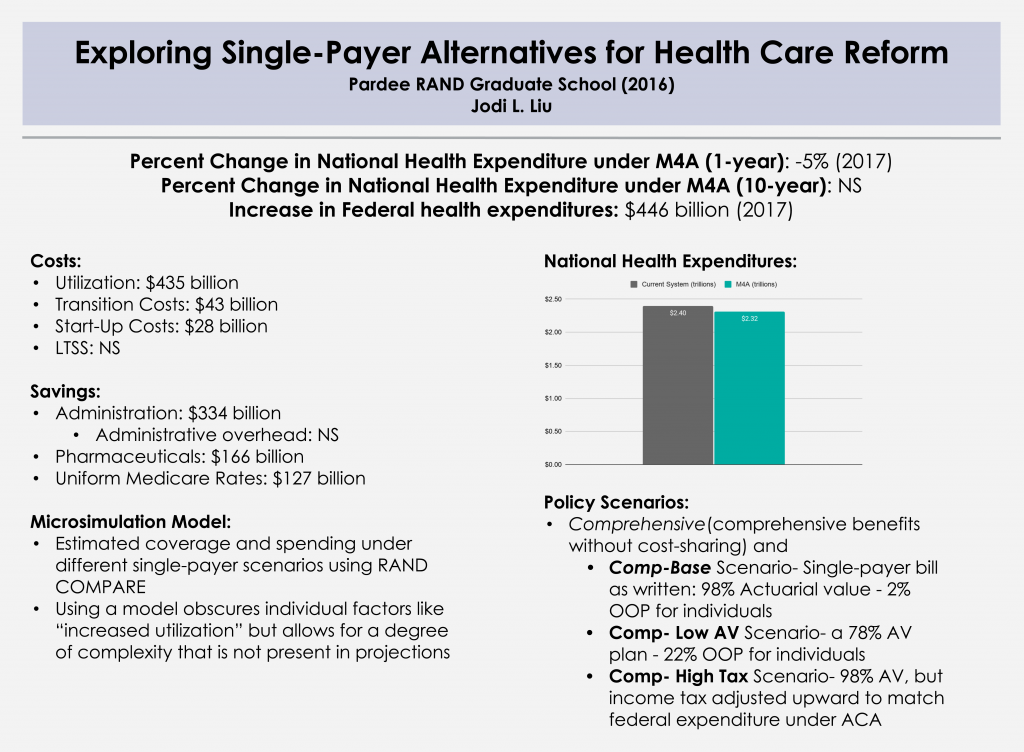
Title: Exploring Unmarried-Payer Alternatives for Health Care Reform
Yr: 2016
Authors: Jodi Fifty. Liu
Institution: Pardee RAND graduate schoolhouse
Funding Source: North/A
Programme Analyzed: S. 1782 / H.R. 1200
Percent Modify in National Health Expenditure under M4A (ane-year): -5% (2017)
Percent Change in National Health Expenditure under M4A (x-year): NS
Increase in Federal health expenditures: $446 billion (2017)
Read Study:
Exploring Single-Payer Alternatives for Health Care Reform
Study Abstract:
The Affordable Care Human activity (ACA) has reduced the number of uninsured and established new cost containment initiatives. However, interest in more comprehensive health care reform such equally a single-payer system has persisted. Definitions of single-payer systems are heterogeneous, and estimates of the effects on spending vary. The objectives of this dissertation were to understand single-payer proposals and to estimate health intendance spending under unmarried-payer alternatives in the United States. Unmarried-payer proposals are wide-ranging reform efforts spanning financing and commitment, but vary in the provisions. I modeled two sets of national scenarios – one labeled comprehensive and the other catastrophic – and compared insurance coverage and spending relative to the ACA in 2017. Kickoff, I estimated the furnishings of utilization and financing changes, and so I added the effects of "other savings and costs" relating to administration, drug and provider prices, and implementation. Due to coverage of all legal residents and low cost sharing, and prior to adjusting for other savings and costs, the comprehensive scenario increased national wellness care expenditures past $435 billion and federal expenditures past $i trillion relative to the ACA. The range of the net outcome of the other savings and costs in the literature was $1.v trillion in savings to $140 billion in costs, with a mean judge of $556 billion in savings. If this mean gauge was practical to the comprehensive scenario, national expenditures would exist $121 billion lower but federal expenditures would all the same exist $446 billion higher relative to the ACA. The catastrophic scenario as well covered all legal residents but increased overall toll sharing, resulting in a reduction in national expenditures by $211 billion and federal expenditures past $twoscore billion even before adjusting for other savings and costs. Average household spending on health care in both sets of scenarios could be more progressive by income than spending nether the ACA. I likewise developed an interactive, spider web-based cost tool that allows the savings and cost assumptions to exist adjusted by any user. Equally the debate on how to finance health intendance for all Americans continues, this study provides increased transparency about economic evaluations of health intendance reform.
Overview:
- This comprehensive 2016 paper served every bit Jodi Liu's dissertation, which utilizes a microsimulation model to account for costs/savings and private level variation
- The newspaper contains iv main chapters:
- Affiliate 1: A review of types of health care systems, single-payer systems worldwide, and brief overview of single-payer health care reform in the Usa
- Chapter 2: Definitions of single-payer health care systems and a survey of single-payer proposals
- Chapter 3: Estimates of health insurance coverage and spending under single-payer scenarios
- Liu looks at 2 policy scenarios: Comprehensive (comprehensive benefits without cost-sharing) and Catastrophic (coverage only against large financial loss)
- Comp-Base of operations Scenario – Single-payer neb equally written: 98% Actuarial value (2% OOP for individuals)
- Comp-Low AV Scenario – a 78% AV plan (22% OOP for individuals)
- Comp-High Taxation Scenario – 98% AV, but income tax adjusted upward to friction match federal expenditure nether ACA
- Affiliate iv: Description of a cost tool that could be used to empathize assumptions (non available)
"Funding HR 676: The Expanded and Improved Medicare for All Deed"
University of Massachusetts at Amherst 2013
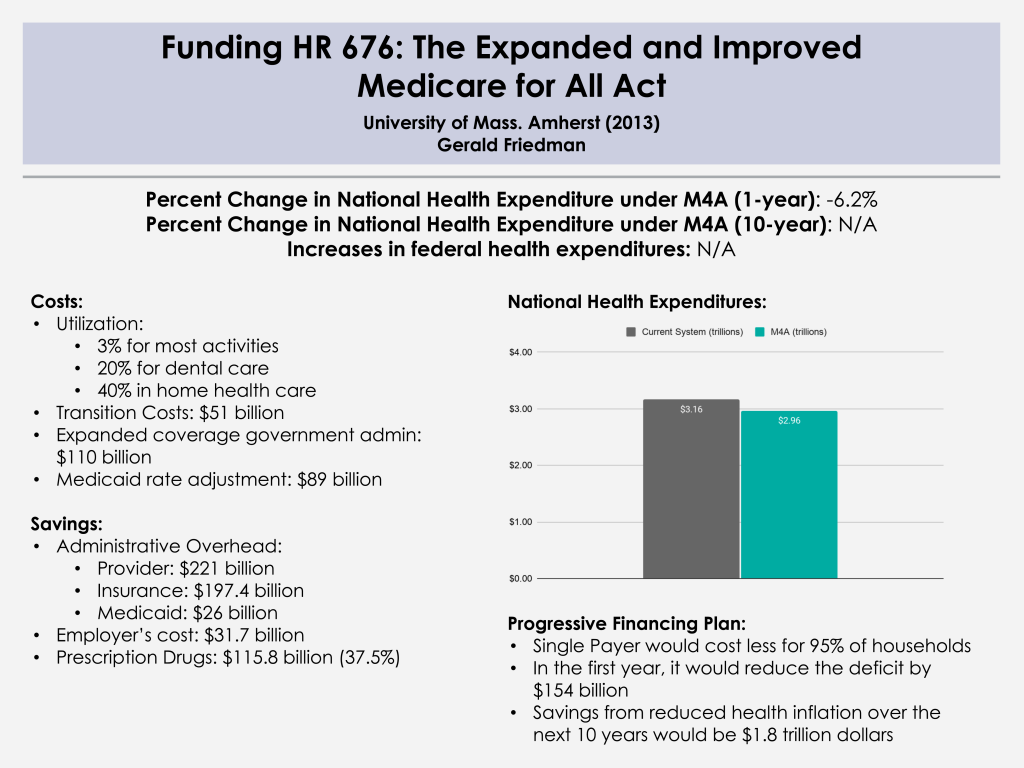
Championship: Funding HR 676: The Expanded and Improved Medicare for All Act
Year: 2013
Author: Gerald Friedman
Institution: University of Massachusetts at Amherst
Plan Analyzed: H.R. 676
Percent Change in National Health Expenditure under M4A (i-twelvemonth): -half dozen.2% (2014)
Read Study:
Funding HR 676: The Expanded and Improved Medicare for All Act
Abstruse:
The Expanded and Improved Medicare for All Act, 60 minutes 676, introduced into the 113th Congress by Rep. John Conyers Jr. and 37 initial co-sponsors, would establish a unmarried say-so responsible for paying for medically necessary health care for all residents of the United states. Under the single-payer system created by Hr 676, the U.S. could salve an estimated $592 billion annually by slashing the administrative waste associated with the individual insurance industry ($476 billion) and reducing pharmaceutical prices to European levels ($116 billion). In 2014, the savings would exist plenty to embrace all 44 million uninsured and upgrade benefits for everyone else. No other plan tin can reach this magnitude of savings on health care. Specifically, the savings from a single-payer program would be more than enough to fund $343 billion in improvements to the health system such as expanded coverage, improved benefits, enhanced reimbursement of providers serving indigent patients, and the elimination of co-payments and deductibles in 2014. The savings would also fund $51 billion in transition costs such as retraining displaced workers and phasing out investor owned, for-profit delivery systems. Health care financing in the U.S. is regressive, weighing heaviest on the poor, the working class, and the ill. With the progressive financing plan outlined for Hr 676 (below), 95% of all U.S. households would save money. HR 676 would also found a arrangement for future cost control using proven-effective methods such as negotiated fees, global budgets, and capital planning. Over time, reduced health toll inflation over the side by side decade ("angle the cost curve") would save $1.8 trillion, making comprehensive health benefits sustainable for futurity generations.
Overview:
Dr. Friedman conducts an easy-to-follow toll analysis of H.R. 676 using a projection model. Dr. Friedman likewise discusses financing this program through both existing funding sources and "progressive tax."
- Section I: Financing needs for single payer
- Current regressive and obsolete funding sources to be replaced by progressive revenue enhancement
- Estimated costs of organization improvements and transition costs
- Section Two: Single-payer system savings as a source of financing
- Savings on provider administrative overhead and drug prices
- Savings on the authoritative overhead of private insurers, Medicaid, and employers
- Section Iii: A progressive financing plan for HR 676 for 2014
- Conclusion: Single payer covers more than, costs less for 95 per centum of Americans
Further Reading:
Gordon Mosser Critical Review and annotate by Dr. Don McCanne
back to topSource: https://pnhp.org/financing-a-single-payer-national-health-program/
Posted by: marineyoune1946.blogspot.com
0 Response to "Where Would The Money Come From For Single Payer Healthcare"
Post a Comment